Muscle Knots (Trigger Points) and Adhesions

Muscle Knots (Trigger Points) and Adhesions: How They Form and Why They Hurt
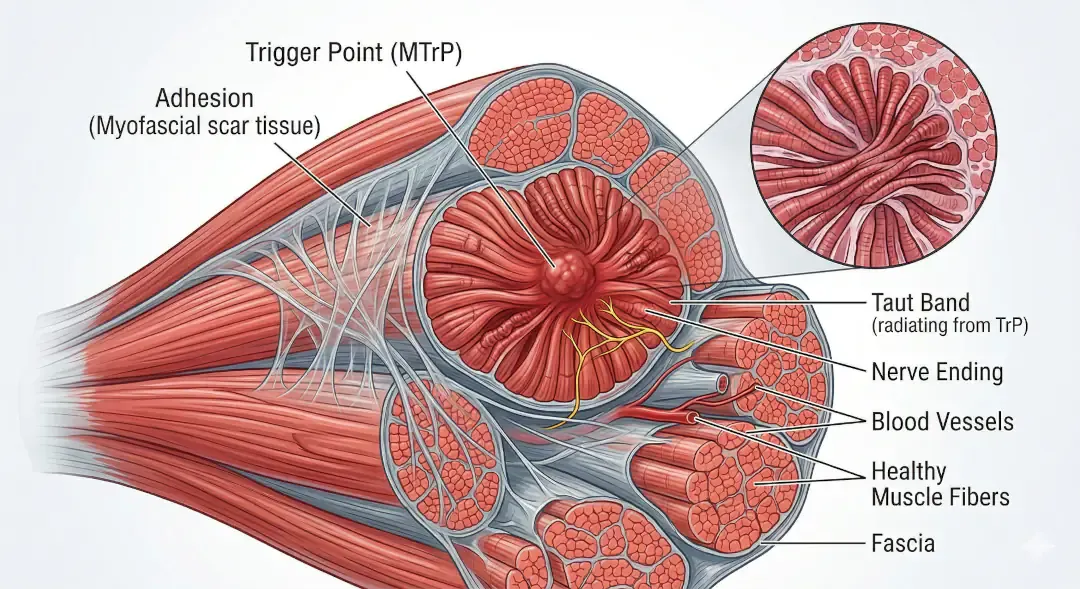
Muscle knots technically called myofascial trigger points form when overuse, stress, or dehydration causes a small group of muscle fibers to remain contracted. Imagine a tiny cramp that won't let go: the muscle fibers squeeze down on nearby blood vessels, cutting off oxygen and trapping waste products like lactic acid. This chemical irritation irritates nearby nerves, creating that deep, aching pain we all recognise. Movement, stretching, and better circulation eventually help the fibers relax but sometimes they need a little help.
The Role of Fascia and Adhesions
While knots involve muscle fibers, adhesions are stickier problems. As I have mentioned in a previous blog, your body is wrapped in fascia a thin, tough web of connective tissue that surrounds every muscle, nerve, and organ. It's like clingfilm. Healthy fascia glides smoothly, allowing tissues to move freely. But when inflammation, injury, or repetitive strain occurs, fascia can develop internal "stickiness" where collagen fibers cross-link and glue layers together. These adhesions restrict movement, disrupt how your body naturally moves, and create compensatory patterns that overload other areas. Unlike knots, which feel like tender lumps when pressed, adhesions often show up as widespread stiffness or a pulling sensation that seems to travel along lines of tension.
The Self-Perpetuating Pain Cycle
Both knots and adhesions thrive on stagnation. Research reveals that trigger points create a vicious metabolic cycle: the sustained contraction compresses blood vessels, causing oxygen starvation and energy depletion. Without fuel, the muscle's calcium pumps fail, trapping fibers in contraction and allowing waste products to accumulate. This toxic buildup activates pain receptors and releases inflammatory chemicals that make nerve endings even more sensitive.
Scientists call this the "Cinderella hypothesis" smaller muscle fibers used for sustained tasks (like holding your phone or sitting at a desk) work the hardest and rest the least, making them most vulnerable to getting stuck.
Why Pain Spreads
The pain doesn't stay local. Constant signals from trigger points make nearby nerve endings hypersensitive a process called peripheral sensitisation. More significantly, persistent pain signals rewire the spinal cord itself through central sensitisation, where pain neurons become hyperactive even after the original trigger quiets down.
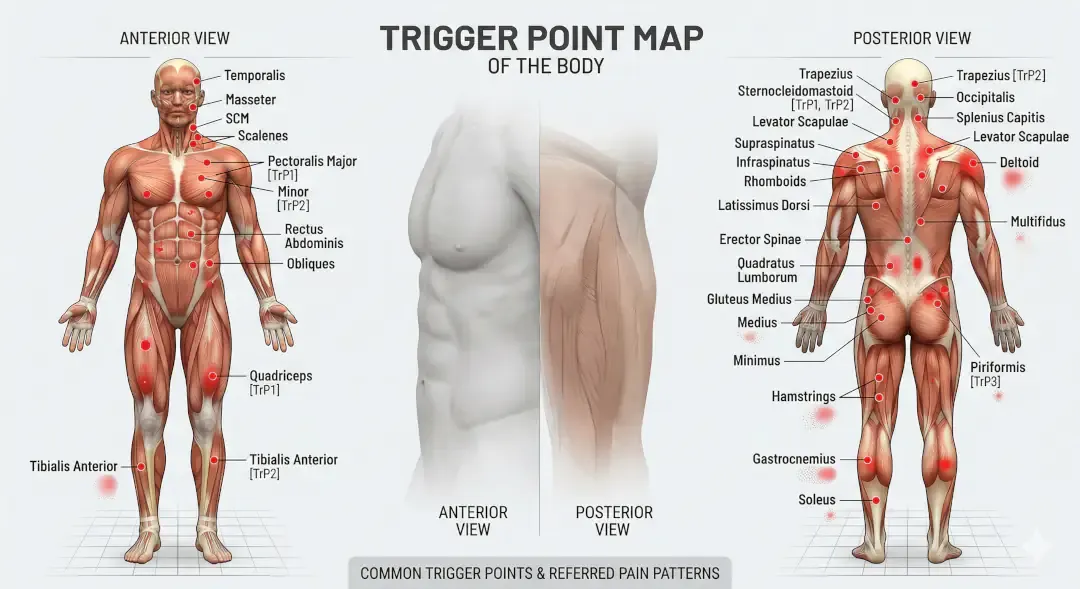
This explains why your shoulder knot triggers headaches, or why hip stiffness shows up as knee pain. Studies show that latent trigger points ones that don't hurt until pressed constantly send low-level signals to the spinal cord, priming your nervous system to overreact. Stress chemicals like serotonin and norepinephrine build up in the area. Both send pain signals to your brain and keep muscles tense so pain makes the muscle tighter, which creates more pain, which makes it tighter still.
Practical Self-Treatment
Breaking the cycle means restoring movement and circulation. Here's what actually works:
Hydration first. Fascia is mostly water; dehydration makes it stiff and prone to sticking. Aim for consistent fluid intake throughout the day, not just chugging when you remember.
Movement as medicine. Gentle, pain-free range-of-motion exercises pump fluid through tissues and reset neuromuscular tone. Think simple yoga stretches, shoulder rolls, or simply walking especially after sitting.
Targeted pressure. Foam rolling, massage balls, or simply pressing on knots with your fingers briefly squeezes the area, cutting off blood flow. When you release the pressure, fresh blood rushes back in like a dam opening flooding the tissue with oxygen and nutrients that help the muscle fibres finally let go. Spend 30-90 seconds on tender spots, breathing deeply until intensity drops.
Heat therapy. Warmth increases blood flow and tissue pliability. Use before stretching or self-massage for best effect.
Posture breaks. Set timers to move every 30-45 minutes. The Cinderella fibers need regular recruitment changes to prevent metabolic stagnation.
Sleep and stress management. Poor sleep and chronic stress crank up brain chemicals that keep muscles tense, keeping the whole pain cycle spinning.
When to Seek Help
Self-treatment works for recent, uncomplicated knots. But if pain persists beyond a few weeks, spreads significantly, or follows injury, consult a professional. Physical therapists can access deeper layers, break established adhesions, and address the central sensitisation component that self-care often misses.
Conclusion
Muscle knots and adhesions aren't just annoying they're real physical problems involving stuck tissue, energy starvation, and an oversensitive nervous system. The upside? This means there are many ways to fix them.
Prevention is straightforward: drink water, keep moving, and manage stress. These habits stop the problem before it starts. When knots do appear, simple self-treatment can break the pain cycle early.
It's also worth knowing that pain often spreads beyond the original spot. That shoulder ache might involve your spinal cord, not just the muscle itself. This means treating the wider picture not just the tender spot gives better results.
Your body isn't punishing you. Pain is a genuine signal that something needs attention. Act early, keep it simple, and stay active
References
https://pmc.ncbi.nlm.nih.gov/articles/PMC11266154/
Shah JP, Danoff JV, Desai MJ, et al. Biochemicals associated with pain and inflammation are elevated in sites near and remote from active myofascial trigger points. Arch Phys Med Rehabil. 2008;89(1):16-23.
https://pmc.ncbi.nlm.nih.gov/articles/PMC4508225/
Gerwin RD, Dommerholt J, Shah JP. An expansion of Simons' integrated hypothesis of trigger point formation. Curr Pain Headache Rep. 2004;8(6):468-475.
https://pubmed.ncbi.nlm.nih.gov/24264721/
Fernández-de-Las-Peñas C, Dommerholt J. International consensus on diagnostic criteria and clinical considerations of myofascial trigger points. Arch Phys Med Rehabil. 2018;99(1):144-155.